What is CBT for insomnia?
- CBT-I helps rebuild a healthy relationship with sleep by addressing negative thoughts and behaviors.1,2
- Five main aspects: sleep hygiene, stimulus control, sleep restriction, relaxation training, and cognitive therapy.3
- Benefits and limitations of cognitive behavioral therapy in the treatment of insomnia.
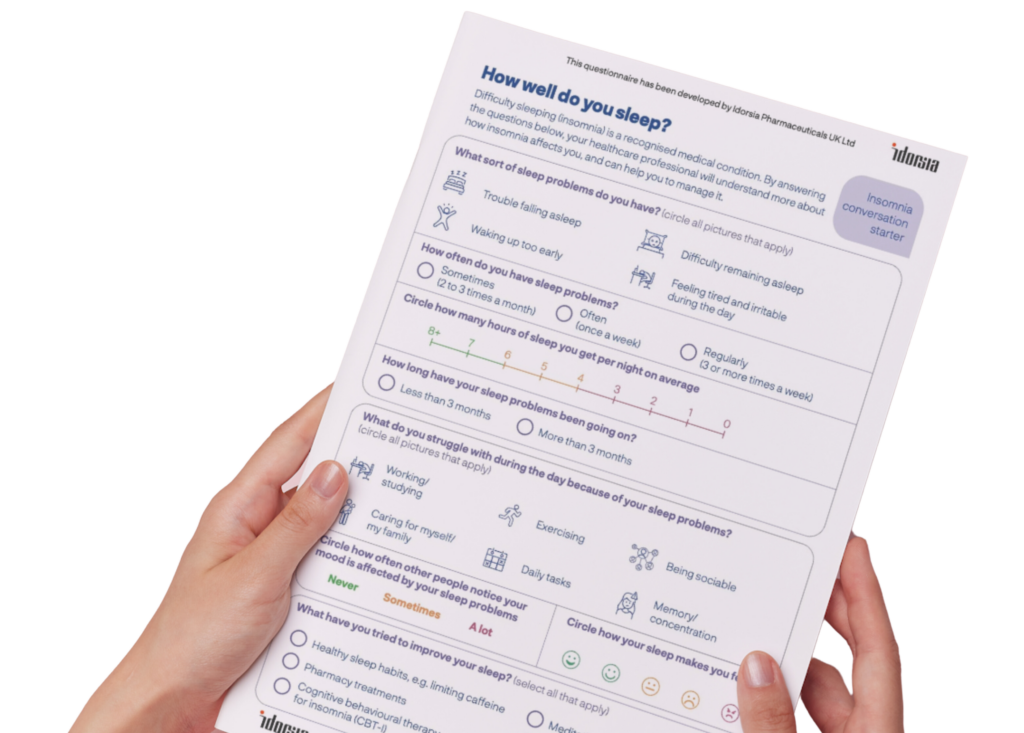
Before we get started, why don’t you find out more about
your relationship with sleep and how it affects your days and nights?

Everyone has trouble sleeping now and then. But when trouble sleeping becomes something that lasts for at least 3 times a week for 3 months or longer, it’s known as chronic insomnia.4

Poor sleep also affects your daytime activity. If you don’t get enough restful sleep at night, it can result in:4
- Morning sleepiness
- Fatigue
- Bad work performance
- Reduced social interactions
- Poor concentration
- Irritability and bad moods
We know what may be behind chronic insomnia
If you’re interested in cognitive behavioral therapy for insomnia (CBT-I) and want to know more about it, you’re in the right place.
Here, you can find out how it works, how it may help your insomnia and the overall pros and cons.
CBT-I is a way of building back a better, healthier and happier relationship with sleep. It does this by helping you see the bedroom through a new lens as a calming and inviting space, rather than a disruptive one.5
For CBT-I to work, it takes commitment, time and effort.5
If you try CBT for insomnia, how does it work?
Let’s set the scene.
You’ve lived with chronic insomnia for months, or even years, and you don’t look forward to going to bed like most other people do.2
Night-time becomes a challenge or even a chore, because the parts of the brain which should be in sleep mode are instead still active – keeping you awake.6
Not getting enough restorative sleep can leave you feeling exhausted and tired during the day, and knowing this can trigger a negative cycle of anxious thoughts before bedtime.1
Nobody wants that, do they?
And, if you start to make this link in your mind that going to bed means you’re going to be wide awake and alert, you may start acting that going to bed means you’re going to be wide awake and alert, you may start acting differently before getting into bed.3 Certain behaviours before bedtime can fuel an overactive brain, which can make it even harder for you to fall asleep.2
This is where CBT-I comes in
It’s a type of psychotherapy that helps to reduce any negative thoughts and worries surrounding sleep you may have by suggesting ways to improve your sleep habits and behaviours.2
The treatment is practical and structured. You work with a therapist to break the negative cycle of thoughts about night-time and train your brain to see sleep as a good thing once again.2
CBT-I is recommended as a first line treatment for people living with chronic Insomnia.6 There are lots of different approaches and 6 to 8 sessions are usually required if you want to reap the long-term rewards.2
So what does CBT for insomnia consist of?
There are 5 main aspects to CBT for insomnia:3
1. Sleep hygiene
You create a calm and comfortable bedroom environment that’s supported by a sustainable night-time routine to help you wind down at the end of a long day. Maybe it’s only changing into your pyjamas when it’s bedtime, restricting stimulants, like caffeine, in the afternoon, avoiding daytime napping, or settling down with a good book for a while before turning in.
It’s all about what works best for you.3
2. Stimulus control
You restrict your time in bed, so it’s mainly used for sleep. You’ll also banish blue light stimulation from devices like laptops and phones from the bedroom. You can keep them in another room but if you typically use your phone as a morning alarm, you might need to invest in an old-fashioned alarm clock!3
3. Sleep restriction
You only get into bed when you are ready to go to bed and fall asleep. That’s it. When you’re up, you’re not in the bedroom. When you want to go to sleep, you can come back in.3
4. Relaxation training
You take part in some exercises that help you relax both your body and your mind before bedtime. Think of lots of deep breaths, in through the nose and out through the mouth.3
5. Cognitive therapy
You dig deep by identifying, challenging, and altering the way you see your sleep. This is you getting to the root cause of your bad bedroom relationship. The aim is simple: change negative perceptions about sleep to help reduce stress, anxiety and worries in the time leading up to bedtime.3
Benefits and limitations of cognitive behavioral therapy
in the treatment of insomnia
- CBT-I has shown to have long term benefits even after you stop therapy or finish your course7
- It’s a non-pharmacological treatment
- Some people find CBT-I is better at improving daytime symptoms of chronic insomnia like fatigue and lack of concentration7
- CBT-I needs 6 to 8 total sessions of therapy, and you need to build the habit of using a sleep diary so you can monitor changes in your sleep over time.5 This can be time consuming and tricky to schedule in if you’re already having difficulty with your work-life balance
- CBT-I is not a treatment that is easily accessible for everyone due to costs and the time it needs
Final thoughts on CBT-I
You may find that you behave differently, compared to when you didn’t have insomnia, when you try to go to bed. CBT for insomnia aims to rebuild your relationship with sleep.
It has a number of different approaches, is a non-pharmacological form of treatment, and some people see lasting results after they complete a course.5,7
That being said, CBT-I takes a lot of time and some dedication, and not everyone is able to access this form of treatment.
Ready for a fresh conversation about chronic insomnia?
References
1. Killgore W. Neuroreport. 2013; 24(5):233–40.
2. Koranyi N, et al. J Sleep Res. 2018; 27(2):215–219.
3. Fang H, et al. J Cell Mol Med. 2019; 23(4): 2324–2332.
4.Reimann D, et al. J Sleep Res. 2017; 26(6): 675–700.
5.Anderson K. J Thorac Dis. 2018; 10(Suppl 1): S94–S102.
6. Riemann D, et al. Sleep Med Rev. 2010; 14(1):19–31.
7. Davidson J. Br J Gen Pract. 2019; 29;69(686):e657-e664.
EUC-IDS-00086 April 2025